
 In a recent review published in Nutrients, researchers assessed nutrition-related studies involving sickle cell disease (SCD) patients, particularly those in Africa.
In a recent review published in Nutrients, researchers assessed nutrition-related studies involving sickle cell disease (SCD) patients, particularly those in Africa.
The study found that nutritional deficiencies contribute to SCD severity, increasing interest in dietary supplements. SCD patients require more calories and protein, and malnutrition is a typical consequence.
Omega-3 fatty acids, notably DHA and EPA, are potent anti-inflammatory mediators in SCD that control pain and reduce Vaso-Occlusive Crisis (VOC) episodes.
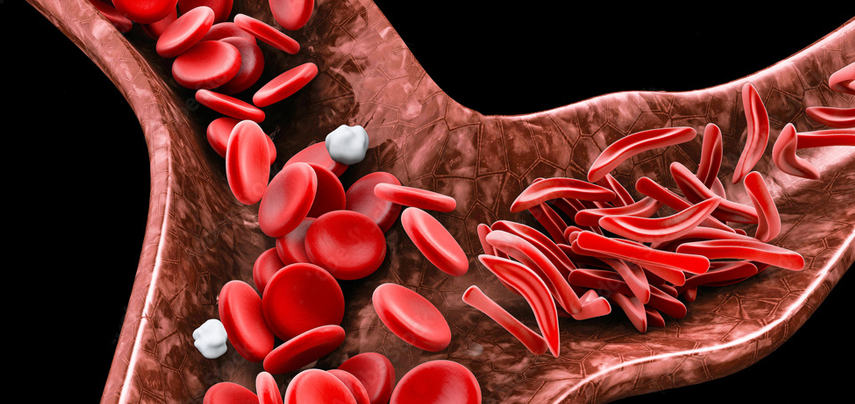
A vaso-occlusive crisis, or VOC, occurs when sickled red blood cells block blood flow to the point that tissues become deprived of oxygen. This in turn sets in motion an inflammatory response as the body tries to rectify the problem.
Polyunsaturated omega-3 fatty acids have been demonstrated to be helpful in SCD in clinical studies.
The three main omega-3 fatty acids are alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). ALA is found mainly in plant oils such as flaxseed, soybean, and canola oils. DHA and EPA are found in fish and other seafood.
Antioxidant-rich edible mushrooms have several pharmacological effects and can improve health, lifespan, and quality of life.
Ganoderma lucidum reduces hemoglobin polymerization rate; Auricularia auricular scavenges free radicals; Hericium erinaceus regulates heat shock proteins; and Termitomyces increases hemoglobin levels and white blood cells.
Commonly known as reishi mushroom, Ganoderma lucidum is a purple-brown fungus with a long, thin stalk, spores that are brown in color and a shiny cap shaped like a fan. The mushroom grows on decaying logs and tree stumps. While Ganoderma lucidum is indigenous to North America, Japan and China, it is produced in a number of other Asian countries.
Phytochemical analysis showed it has one active ingredient, polysaccharides, which contain beta glucan. Beta glucan is known for its ability to enhance the immune system – in fact it is one of the strongest immune system supplements there is.
Another ingredient in ganoderma is triterpenes. The type found in ganoderma is a ganoderic acid that has been proven in studies to ease the symptoms of allergies by stopping the release of histamines. It also can improve the body’s use of oxygen and help the liver function better.
Until now, Ganoderma mushroom is used in various systems of traditional medicine for the treatment of a plethora of diseases.
Systematic pharmacological and clinical studies suggest that Ganoderma is useful in the treatment of coronary heart diseases, arteriosclerosis, hepatitis, arthritis, nephritis, bronchitis, asthma, hypertension, cancer and gastric ulcer. The most important pharmacologically active constituents of Ganoderma lucidum are triterpenoids and polysaccharides.
Triterpenoids have been reported to possess hepato-protective, anti-hypertensive, hypocholesterolemic and anti-histaminic effects, anti-tumour and anti-engiogenic activity, effects on platelet aggregation and complement inhibition.
Polysaccharides, especially b-Dglucans, have been known to possess anti-tumor effects through immunomodulation and antiangiogenesis. In addition, polysaccharides have a protective effect against free radicals and reduce cell damage caused by mutagens.
Meanwhile, according to the review, in Africa, integrating natural and pharmacological therapy is critical for SCD management. Traditional healers use up to 5,000 native medicinal foods gathered from plants, benefiting over 80 per cent of Africans.
Conventional treatments have higher popularity than modern medications; however, they may be lost to future generations due to verbal transmission. Tropical plant bioactive chemicals interact with phytonutrients and gut bacteria, playing a crucial regulatory function in human wellness.
Researchers have investigated nutritional advantages in individuals with SCD in Nigeria, with limited studies in other nations of Sub-Saharan Africa. Indigenous medicinal substances include seed oils obtained from Ipomoea involucrata, Solenostemon monostachyus, Cajanus cajan, Acacia Senegal, and Carica papaya (pawpaw).
Solenostemon monostachyus belongs to the plant family Lamiaceae, and is commonly named African dead nettle. It is called Ntorikwot in Efik.
Botanically called Cajanus cajan, Pigeon pea belongs to the plant family Leguminosae (Fabaceae). In Nigeria, it is called fio fio in Igbo, waken-masar or waken-turawa in Hausa, and otili or otinli in Yoruba.
Ceiba pentandra and Alchornea cordifolia are used medicinally in the Democratic Republic of the Congo to prepare the “blood tonic” beverage.
Ceiba Pentandra belongs to the plant family Bombacaceae. It is commonly called silk cotton tree, kaboka tree; Akpu-ogwu in Igbo; Rimi in Hausa; Ogun- gun, Araba in Yoruba.
Botanically called Alchornea cordifolia, it is called oje in Ebira-Etuno; uwonmwe in Edo; mbom in Efik; tahi in Gwari; bambani or bombana in Hausa; ubebe or ububo in Igbo; ipain in Ijaw; ukpaoromi in Yekhee; and epa or ipan-esin in Yoruba.
Moringa oleifera, high in phytochemicals with anti-urolithiasis characteristics, is used to treat SCD and Nigella sativa due to its antioxidant qualities.
The researchers concluded: “The review findings highlighted therapeutic approaches for sickle cell disease, a condition causing dysfunctional immune responses.
“The findings indicate nutritional interventions for patients, especially those residing in the sub-Saharan regions of Africa, and emphasize the need for increasing clinical nutrition research to optimize SCD management, including medicinal plants.
“Nutritional treatments can improve overall well-being, and encouraging functional diets can help to prevent crises. In SCD, microbiota modification can correct microbial dysbiosis, and omega-3 fatty acids can enhance VOC rate, inflammatory indicators, adhesion, and hemolysis.
“African plants like Alchornea cordifolia and Ceiba pentandra make blood tonics; Moringa oleiferafor its anti-urolithiasis effects; and Nigella sativa and Carica papaya for their antioxidant characteristics.
“Mushrooms can lower the rate of hemoglobin polymerization, scavenge free radicals, control heat shock proteins, and boost hemoglobin levels and white blood cell counts.”
Commonly called black seed, Nigella sativa belongs to the plant family Ranunculaceae. It is a widely used medicinal plant throughout the world.
SCD, a congenital blood condition, is common in affluent nations, although statistics on frequency, morbidity, and death are lacking. Medical treatment in impoverished regions includes hydroxyurea, blood transfusions, and painkillers.
Nutrition treatments are essential to deal with increasing nutritional expenditures and supportive management. To sustain well-being and quality of life, underprivileged regions in Sub-Saharan Africa must optimize the dietary regulation of SCD.
While plant resources are recognized, researchers have exploited only a few herbal methods and products.
In the present review, researchers reviewed nutritional approaches to treat SCD.
Aberrantly polymerized deoxygenated hemoglobin, formed by polymerizing two mutant sickle β-globin subunits, causing red blood cell deformation, produces SCD. Hemoglobin beta gene (β-HBB) mutations characterize the congenital disease.
Heme oxygenase 1, a member of the heat shock protein (HSP32) family, causes ferroptosis and sickling of red blood cells. Sickled (crescent-shaped) red blood cells result in a vaso-occlusive crisis (VOC), which occurs in case of blood flow obstruction that deprives tissues and organs of oxygen.
SCD complications include infections, aches and pains, retinopathy, nephropathy, and cerebrovascular accidents.
Blood transfusions, hydroxyurea to increase fetal hemoglobin, hematopoietic stem cell transplantation to reverse the sickle phenotype, L-glutamine for antioxidant effects, hemoglobin S polymerization inhibitors to prevent hemoglobin S (HbS) polymerization, monoclonal antibodies like crizanlizumab to reduce sickle-mediated adhesion, and clustered regularly interspaced short palindromic repeats (CRISPR)-associated protein 9 (Cas 9) gene-editing therapies to edit faulty genes in bone marrow stem cells are among the therapeutic interventions.
Allogeneic hematopoietic stem cell transplantation is the only confirmed treatment option for SCD, ideally from an unaffected human leukocyte antigen (HLA)-identical sibling donor. Combining genetic therapies with hydroxyurea yields the best outcomes but is usually reserved for children under the age of 16 who have significant problems.
Increased gut damage, permeability, altered microbiota composition, and bacterial overgrowth occur in SCA. In SCD patients, this dysbiosis causes inflammation and suffering.
The human genome influences the gut microbiome through enzymes and micro-ribonucleic acids (miRNAs), and microbiota modulation tries to reverse established microbial dysbiosis.











