 Follow Us on Google News
Follow Us on Google News Follow Us on Google Discover
Follow Us on Google Discover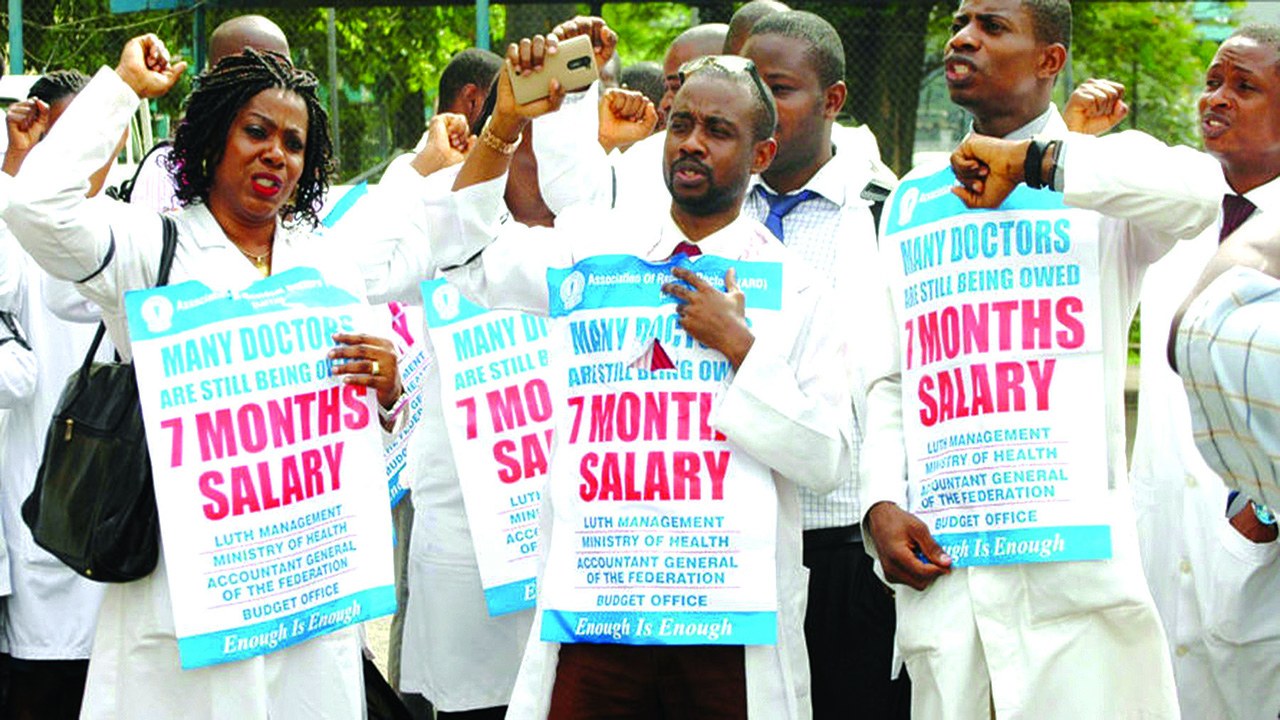
[vvideo code=”XGQYXY0F” autoplay=”yes”]
There is anxiety over Nigerian doctors leaving town en masse. According to a recent report, Saudi Arabian officials interviewed in Abuja more than 200 medical personnel seeking placements in the Gulf nation.
Observers have acknowledged that Nigeria does not have enough doctors to meet the need of its population.
Yet, they are unable to comprehend why trainee doctors find it hard to get places to do internship.
[ad]
Figures released February 2018 by the British government indicate that no fewer than 5,405 Nigerian-trained doctors and nurses are currently working with the British National Health Service (NHS) in the United Kingdom (U.K.).
This means that Nigerian medics constitute 3.9 per cent of the 137,000 foreign staff of 202 nationalities working alongside British doctors and nurses.
The Guardian investigation revealed that more Nigerian doctors would join their colleagues soon. The U.K. has need for medics from Commonwealth countries, since some doctors in the European Union (E.U.) are already leaving on account of Brexit.
[related ids=”610917,611299,611809″]
It was gathered that many Nigerian doctors and nurses are leaving for the U.K. because of better conditions of service.
An unconfirmed report earlier in the year claimed “over 100 doctors have resigned from University College Hospital, Ibadan, this year and 100 from public hospitals in Lagos this month alone.
Similarly, 70 per cent of young Nigerian Doctors are making plans to leave for foreign lands and are taking exams to that effect.”
Reports claim that 660 persons wrote the Professional Linguistic Assessments Board (PLAB) exams, recently, and over 1000 have registered for the next PLAB exam.
The British Council administers the PLAB exams on behalf of the United Kingdom’s (UK’s) General Medical Council.
The PLAB test is the main route by which international medical graduates demonstrate that they have the necessary skills and knowledge to practice medicine in the U.K.
The PLAB examinations are now being conducted in Nigeria, with other countries coming around to conduct interviews and lure away our dispirited doctors.
A Consultant Urological Surgeon with the University of Benin School of Medicine and Teaching Hospital, Dr. Samuel Osaghae, and a Consultant Neurological Surgeon, Brain and Spine Surgery Consortium, Abuja, Dr. Biodun Ogungbo, recently, lamented the absence of robust practice environment to keep doctors within the shores of the country.
Figures from the Nigerian Medical Association (NMA) showed that about 45,000 doctors are currently practicing in Nigeria.
This means that 12 per cent of 45,000 Nigerian doctors, that is 5,405, are practising in the U.K. and the country is now left with less than 40,000, excluding those practising in the U.S., South Africa, Saudi Arabia and others.
NMA President, Dr. Mike Ogirima, described the exodus as worrisome. He said the trend has worsened the doctor-patient ratio of 1:4,000, caused longer waiting time at hospitals, rise in fatal disease outcomes, and more frequent medical errors by over worked doctors.
“Nigeria is using her resources to train doctors and professionals that will leave to work in foreign countries. What are those things attracting these professionals outside? Can we duplicate them here?” asked Ogirima.
Consultant Public Health Physician, Prof. Akin Osibogun, however, said the situation could be reversed if the Federal Government makes the National Insurance Scheme (NHIS) compulsory for all citizens.
According to him, this would provide enough funds to improve the conditions of service and working environment for health professionals.
He said: “The few ones we have are leaving because of poor conditions of service, working environment and after service package.
It means the physician-patient ratio has worsened, maybe from 1:3,000 to 1:5,000. When you compare, those countries that have better physician-patient ratio have better treatment outcomes.”
Osibogun, a former Chief Medical Director (CMD) of the Lagos University Teaching Hospital (LUTH), said Nigeria currently produces about 3,000 medical doctors every year and needs to increase the ratio by producing more, and developing plans on how to retain them.
He explained: “We need to make working conditions attractive. If they know they will have a house after 20 years of training, the lure to leave would be reduced. What are the benefits attached to the job?
What are the provisions for the doctors’ family? What are the long-term prospects for the staff?
“We need to improve the work environment in terms of financing. Make it work-friendly, not crowding 10 persons in one office.
[ad]
Talk about electricity supply; you come to work and you are scheduled to do a surgery but there is no electricity.
We need to be more drastic; re-organising the way we fund health service. There should be compulsory NHIS that will bring a pool of funds. We have to adopt a more holistic approach.”
The situation is not hopeless said consultant paediatric surgeon and current CMD of LUTH, Prof. Chris Bode. He said the high migration of Nigerian doctors to the U.K. is because some doctors in E.U. countries are leaving because of Brexit and the NHS has opened its gates to doctors from Commonwealth countries.
He, however, stressed that Nigeria needs proper planning to harness the opportunity the situation brings. He said: “A medical degree is an international passport. Because of global competition, many doctors are moving to the U.S. and U.K.
We lose because we trained them. But we also learn from them by getting exposed to cutting-edge technologies. One day, if we harness them, they will come back to impact positively on the practice here.
“That is the method Japan, India and China used in adapting what they learnt in the U.S. and U.K. It is not a total loss. We are seeing a lot of movement of medical doctors abroad. It is not as if Nigerian medicine is dead.
I had to spend a lot, $14,000, some years back in going to Israel to learn new skills. That has distinguished me, and Nigerians are benefitting.
“Nigerian doctors are going to the U.K. because they have opened their gates. By the time the medical doctors come back, we will be better for it. It is not a hopeless situation. There is a lot we can do to harness the opportunity. We need proper planning.”
Medical Director, Optimal Specialist Hospital Surulere, Lagos, Dr. Celestine Ugochukwu Chukwunenye, said solving the problem of brain drain is not like analysing the amino acid sequence of protein in the leg of a mosquito.
He said government must take the health sector out of the realm of politics and the public sector, and that each health facility should have its own governing board virtually free of ministerial control.
The consultant gynaecologist said the National Assembly should approve subsidies for Teaching Hospitals based on verifiable criteria of performance. He explained: “The Federal Medical Centres should be handed over to the states.
Each Teaching Hospital should then be allowed to float or sink. Their governing boards should reflect the interest of their catchment area and appropriate pricing of their services in line with available government subsidies.”
Chukwunenye said the NHIS must be strengthened to provide better access to these facilities. According to him, it is a ruse to think that forcing the teaching hospitals to charge fees like Primary Health Centres (PHCs) is the way to improve access to them.
Former President, NMA, and Vice President Commonwealth Medical Association (CWMA), Dr. Osahon Enabulele, recommended: “Better political commitment to health; better appreciation of the worth of medical personnel, along with better and competitive wages/remuneration; better working conditions and inspiring work environment; better security and access to social amenities; attractive and globally respected postgraduate training programmes.”
Furthermore, former Minister of State for Health and Executive Director Primary Health Care Development Agency (NPHCDA), Dr. Muhammad Ali Pate, said the causes of medical doctors trooping abroad for greener pastures are poor governance, financing and accountability within the system.
Pate is currently the Chief Executive Officer of Big Win Philanthropy and an Adjunct Professor of Global Health, Duke University Global Health Institute. He is also a member of the Strategic Advisory Group of Experts.
Pate told The Guardian: “Nigerian health professionals are among the best anywhere in the world. In the course of my work, I have encountered compatriots in far away places like Australia and the Solomon Islands, in Africa as well as Europe and North America. Wherever Nigerian health professionals go, they excel.
“Thus the big question of why they don’t stay at home and equally excel. I believe we can find the answer by examining the worldview, structure and functioning of the Nigerian health system. The reality is that our national health system, despite some recent progress, has many areas that are long overdue for significant reforms.
“We have a mixed health system where both the private and public parts are underperforming. At the root of the problem are leadership, governance, financing and accountability. Private health sector will continue to struggle until we have a substantially improved third party payer for health services.”
Pate said until quality standards are outlined and health workers are enabled to reach those higher care standards, both patients and providers will continue to be disappointed.
He said political leaders, who pay lip service to health care, fail to do the necessary when budget allocations for health are discussed. Instead, they leave for the health systems of better-financed countries, to seek care for themselves and their families.
“If political leaders, who control the public purse, continue to choose to travel abroad for medical care, it is a signal for domestic health workers that they, too, ought to travel abroad in order to practice and advance themselves professionally. We cannot have one without the other,” Pate added.
MEDICAL Director and Chief Executive Officer, Beaconhill Smile Clinics, Dr. Oluwaseun Akinbobola, said though the trend occurs all over the world because of the global nature of the medical profession, the rate in Nigeria is alarming.
He pointed fingers at government’s neglect of medical personnel, and poor and irregular salaries that often result in strike actions. Other reasons, he said, include lack of investment in medical equipment and infrastructure, inadequate security, and disrespect for medical professionals in the country.
On ways to reverse the trend, Akinbobola said: “The leadership of the country must instill confidence in and show willingness to improve healthcare services by signing necessary health acts and bills, increasing funding for the sector and ensuring that funds are properly managed.”
He expressed disappointment that “healthcare is not a priority in our nation, as most decision makers would rather travel abroad when the need arises. Until we prioritise healthcare, I don’t believe this dramatic exodus of doctors will end. You cannot fix a health system you don’t believe in.”
Also, former National President of the Association of General Private Medical Practitioners (AGPMPN), Dr. Anthony Omolola, warned that the brain drain would continue, as long as the atmosphere in which medical practitioners operate is hostile.
He regretted how practitioners, who had just qualified, sometimes struggle to find a place for their mandatory housemanship, even from the medical schools that trained them.
He called for the provision of robust infrastructure in the healthcare system, to enable practitioners get employment with good welfare packages.
[ad unit=2]

