 Follow Us on Google News
Follow Us on Google News Follow Us on Google Discover
Follow Us on Google Discover
For women living with endometriosis, a medical condition that denies a lot of them the opportunity of having their own children, life is unfair. The pain they go through and the tough choice they have to make between having children or not should be of grave concern to all. CHIJIOKE IREMEKA writes on the need for more awareness on this health condition that has forced some women to depend on pain reliving drugs and even become addicted to them.
I Lost My Navel, Everything That Makes Me A Woman – Survivor
If endometriosis were a health condition to be trivialised, Miss Patricia Raymond, a survivor, would have been hale and hearty, and have children to call her own.
The 43-year-old woman had been living with endometriosis pain since her first menstruation at the age of 14, though people around her didn’t know what she was going through. Initially she didn’t know what was happening to her and her parents couldn’t do much to help her situation.
[ad]
She managed to finish her secondary education in pain, missing out, sometimes, in some very crucial school activities due to the excruciating pains of endometriosis. Raymond had to be out of school for some days every month because of her condition. While other female students were in school for four weeks in a month to carry out their academic activities, Raymond would be available in three weeks. She was in this condition until she finished her secondary school and proceeded for her tertiary education.
When Raymond’s family members and friends became aware of her health condition, they were very worried, especially as nobody was able to proffer solution. Wrong reasons were adduced to her state of health.
This disrupted her intimacy with men that came her way, and she has not been married till today in her early 40s.
“I lost everything that made me a woman. I have lived with this pain since my first period at 14 years. The only thing left for me is my faith in God. Nobody understood what I was going through. I wailed, gnashed my teeth, and bled profusely, yet nobody could tell me what my problem was.
“I saw hell and couldn’t stand on my feet. I screamed, when the pain would allow me. In most cases, I couldn’t cry because there was no strength with which to cry. The more I cried, the more pain I felt. It was so painful. It would continue in this manner for the next seven days but the flow was just two to three days.
“I suffered and started living on pain relievers and sleep-inducing pills. I take sleeping pills so that I could, at least, have some rest, but no amount of the pills could stop the pain when it comes. It was the pain that would wake you up in the middle of sleep despite the pills. The pain was so maddening when the pills wear off,” she explained.
Everybody around Raymond, including the doctors, was clueless about what was wrong with her.
“After my secondary school education, I proceeded to tertiary education. I refused to give up. I was able to write my last paper in the university and was taken to the hospital. I graduated, started working and treating myself.
“I had to visit all the gynaecologists I came in contact with, seeking solutions to my condition. When I was taken to the hospital, I did a number of tests and scans but there was nothing found. One of the tests was done in a painful procedure.
“While I was waiting for my turn at the waiting room, I could hear other women going through the same procedure screaming and wailing as if they were being injured. After the tests, nothing was seen because water had taken over my belly at this point, and I was bloated. I went for water draining. After that, I began to shrink. I wondered why professional gynaecologists could not know what I was going through for this long.”
Eventually, in 2003, she had her first surgery. She bled for days and thereafter, started looking for financial assistance to augment her salary to go for treatment. She had lived with the problem for decades. From weighing 69, Raymond went down to 41. At a point, she could neither eat nor drink because she was bloated.
 “I was like a skeleton. I went to the military hospital and started with a Human Immuno Virus (HIV) test and others. I went for a city scan, which cost me N45, 000 but they didn’t see anything because water had taken over my body. I had another surgery, which took away my navel. As I speak, I don’t have a navel because of endometriosis.
“I was like a skeleton. I went to the military hospital and started with a Human Immuno Virus (HIV) test and others. I went for a city scan, which cost me N45, 000 but they didn’t see anything because water had taken over my body. I had another surgery, which took away my navel. As I speak, I don’t have a navel because of endometriosis.
“I have decided to tell my story to help others living with this condition and to create awareness on the need for on-job education for medical practitioners, who were also ignorant of the condition,” she added.
Raymond’s experience is not different from what over 176 million women across the world go through, and this is the reason endometriosis has become a topical issue in recent time to create awareness on the health condition and contribute to the fight against it.
The Guardian learnt that painful mensuration could be a symptom. According to experts, normal menstrual cycle of a lady shouldn’t stop her from performing her normal tasks, but it should be a cause for worry when it does.
It has been reported that between 30 per cent and 40 per cent of Nigerian women who live in Nigeria suffer from endometriosis. There is also a recent study that claims that approximately 11 per cent of women and girls in Nigeria unknowingly live with the disorder, though they show no symptoms, and diagnosis only occur years later.
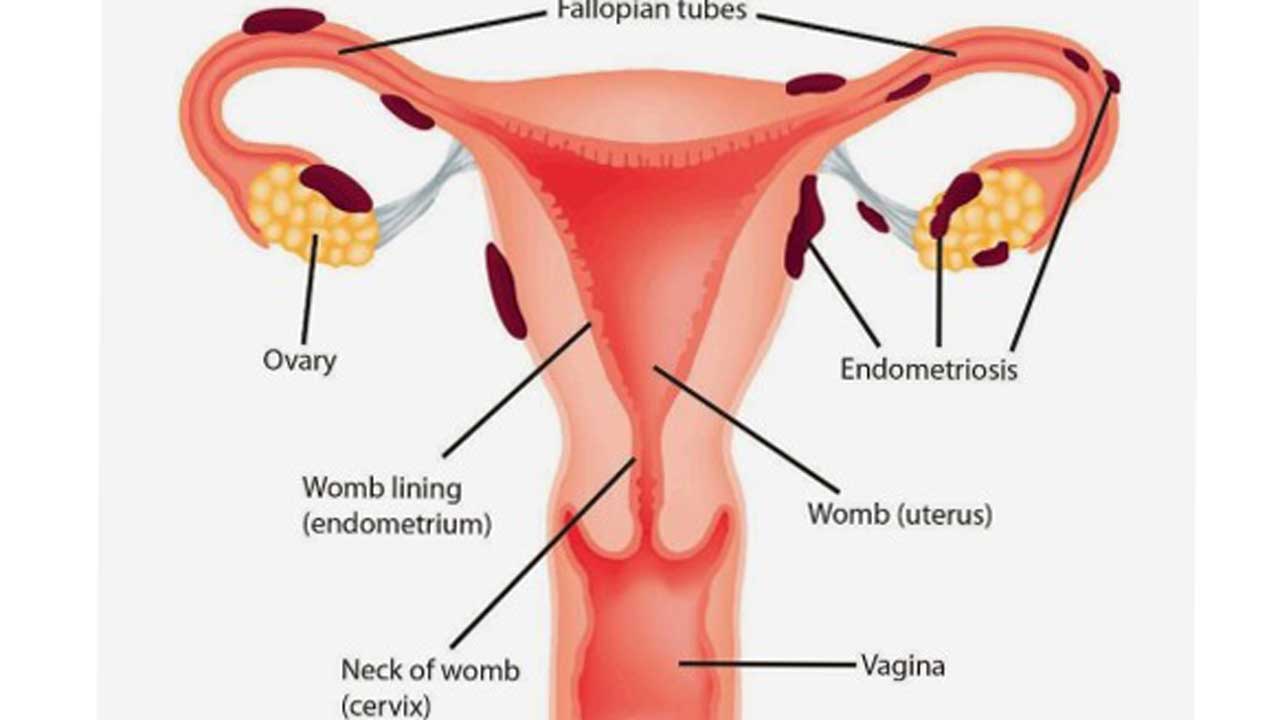
By way of definition, endometriosis is the abnormal growth of cells (endometrial cells) similar to those that form the inside of the uterus, but in a location outside of the uterus. It’s a disorder of the tissue lining the uterus that causes it to grow outside the uterine cavity.
It attaches itself to other organs and swells with blood during menstruation. And since the blood can’t escape, these tissues cysts, and scar tissue or adhesions takes place. This causes pain and prevents the fallopian tube from functioning properly. It affects pregnancy directly.
Recently, a group of professionals from across the world gathered at the Civic Centre in Lagos to educate women and doctors on this condition. The survivors were also there to share their experiences with a view to educating others and giving the survivors hope that they weren’t alone in the struggle. The event brought relief to the survivors after hearing the testimonies of others.
 “I have never met anybody with this condition, if I had, maybe my case wouldn’t have been this complicated. Earlier, I thought I was alone in this condition but today, I feel better. I would appeal that this form of programme should be regularly organised to give us hope and to create awareness for the younger ones. If it will cost me coming here every time to narrate my ordeals to create awareness, I will do it to ensure people don’t go through what I am going through,” Raymond said.
“I have never met anybody with this condition, if I had, maybe my case wouldn’t have been this complicated. Earlier, I thought I was alone in this condition but today, I feel better. I would appeal that this form of programme should be regularly organised to give us hope and to create awareness for the younger ones. If it will cost me coming here every time to narrate my ordeals to create awareness, I will do it to ensure people don’t go through what I am going through,” Raymond said.
[ad]
The experts who were present in person at the event and others who joined via zoom viewed endometriosis as ‘an unrecognised burden in Africa’ that shortens and retards the quality of life of women on the continent.
According to them, one of the reasons the condition is widespread is the ignorance about its existence, especially among women and even some medical practitioners. They said majority of the cases were being detected late when a woman is married and ready for childbearing. This, they said, made many women like Raymond to go experience untold hardship, pain and neglect.
To check the spread of the disease, two advocacy groups, Endometriosis Support Group Nigeria (ESGN) and African Endometriosis Awareness and Support Group (AESG) have been established in Lagos.
Recounting her experience, Botswana-based Gaona Dintwe, who was at the event, said her own condition started with her first menstrual cycle at the age of 14. She suffered misdiagnosis as she was said to have contracted sexually transmitted diseases.
The next time she visited the treatment centre, she was accused of having an abortion because she was bleeding heavily, not knowing she was having endometriosis pain. Dintwe was basically living on drugs until she decided that she shouldn’t be an addict to pain relievers.
“As I am sitting down now, I am in pain but I have to bear it. I have learnt how to ignore the pain not to become an addict. By then, I wasn’t sexually active yet and that was where the misdiagnosis came from. The doctor told me I had an STI even when I did not have sex.
“At that point, I have not tried to make babies but my friend advised me to go for a test. The test proved that one of my fallopian tubes was blocked, but after the surgery the doctor said the chances of having pregnancy was high and that was how I conceived.
“There is no cure for it, you just have to manage the situation, but early diagnosis would help you to manage it effectively,” Dintwe said.
A consultant gynaecologist and obstetrician and the Managing Director, Nordica Fertility Centre, Dr. Abayomi Ajayi, said the aim of the groups, that are being supported by other groups across Africa – Botswana, Lesotho, Zimbabwe, Kenya, South Africa, Ghana and Nigeria– is to raise awareness about the health condition among the people living with it.
[ad]
He listed the major concerns about the condition as inaccurate diagnosis, dearth of trained medical personnel to handle it and obsolete equipment used in medical facilities across the continent.
“For women living with this condition, life seemed very unfair. The pain, the tough choice they have to make in determining if they would have children or not, their sexual life, relationship challenges and general wellbeing should be of grave concern to all of us.
“Up to 50 per cent of women who have this condition may experience infertility. Endometriosis cells secrete substances that affect the sperms and eggs. This causes progesterone deficiency in women and thus preventing normal implantation.
“These implants are most commonly found on the ovaries, the fallopian tubes, outer surfaces of the uterus or intestines, and on the surface lining of the pelvic cavity. They can also be found in the vagina, cervix, and bladder, although less commonly than other locations in the pelvis.
“Rarely, endometriosis implants can occur outside the pelvis, on the liver, in old surgery scars, and even in or around the lung or brain. While they can cause problems, they are not cancerous. Endometriosis affects an estimated 1 in 10 women during their reproductive years, usually between the ages of 15 and 49, which is approximately176 million women in the world,” the doctor explained.
The Guardian learnt that endometriosis could start from as early as a girl’s first period and menopause may not resolve the symptoms, especially if the woman has scar tissue or adhesions from the disease and/or surgery. However, the exact cause of endometriosis has not been identified but it is more common in women who are experiencing infertility than in fertile women. The condition does not fully prevent conception. Endometriosis is the 2nd most common gynaecological condition in Nigeria.
Ajayi also noted that severe endometriosis is often associated with infertility due to the chronic inflammation which occurs as a result of the abnormally positioned endometrial tissue. All endometrial tissues, whether located in the womb or not, respond to the normal hormones that regulate the woman’s menstrual cycles.
On the symptoms of endometriosis, Ajayi mentioned pelvic pain during menstruation or ovulation. He said the symptoms might also occur in normal women. “Cramps, fatigue and painful sex are the major symptoms of this condition.”
[ad]
Endometriosis, he said, can be suspected based on the woman’s pattern of symptoms and sometimes during a physical examination, “but the definite diagnosis is confirmed by surgery, usually laparoscopy.”
According to him, treatment of endometriosis includes medication and surgery for both pain relief and treatment of infertility, if pregnancy is desired.
It was learnt that though endometriosis is associated with inflammation and immunological dysfunctions, it has not been proven itself to be an autoimmune disease.
An autoimmune disease happens when the body’s natural defence system can’t tell the difference between your own cells and foreign cells, causing the body to mistakenly attack normal cells.
Diagnosis
On the diagnosis and management of endometriosis, Dr. Ajayi said a good clinical history and a thorough clinical examination with high index of suspicion help to point in the direction of the correct diagnosis.
“To confirm the diagnosis, it is advised that the patient undergo vagina ultrasound assessment and laparoscopy. A minimal access surgery that employs keyhole camera procedure is considered the ‘gold standard’ tool.
“Laparoscopy also allows for classification of the extent of disease and histological diagnosis. Endometriosis can be managed either with the help of drugs or with surgery. The drugs used for the management are geared towards pain control and reducing the impact of the oestrogen hormone.
“In those with mild to moderate disease, conception can occur spontaneously. Failure to conceive following six to 12 months of trying may necessitate help in the form of assisted conception treatments, mainly invitro-fertilisation.
“Fertility treatment protocols must be tailored to the individual’s need to achieve the desired outcome. The experience revealed that 25 per cent of patients undergoing Assisted Reproductive Technique are affected by endometriosis, and up to 40 per cent of these patients show ovarian endometriosis.
“During endoscopy surgical procedure at Nordica, endometriosis is the third commonest finding (15.7%) at laparoscopy. It is possible for those with endometriosis to live above the pain and achieve their desired goals and aspiration despite the condition.”
[ad]
Dieting
The Guardian learnt that eating more trans fatty acids food could increase the risk of having endometriosis. Also, drinking two or more cups of coffee per day could increase the risk, though some studies found no correlation between the two.
It was gathered that eating more green vegetables and fruits could decrease the risk of endometriosis. Omega-3 fatty acids seem to reduce the risk, just as fish oil intake seems to reduce painful menstruation in some women. Taking three or more servings of dairy food daily decreases the risk of endometriosis.
On how endometriosis leads to infertility in women, a consultant surgeon and gynaecologist with Epe General Hospital, Dr. (Mrs.) Cynthia Okafor said: “Endometriosis can influence fertility in several ways: distorted anatomy of the pelvis, adhesions, scarred fallopian tubes, inflammation of the pelvic structures, altered immune system functioning, changes in the hormonal environment of the eggs, impaired implantation of a pregnancy, and altered egg quality.
“At the time of surgery, your doctor may evaluate the amount, location, and depth of endometriosis and give you a score. This score determines whether your endometriosis is considered minimal (Stage 1), mild (Stage 2), moderate (Stage 3), or severe (Stage 4).
“This scoring system correlates with pregnancy success. Women with severe (Stage 4) endometriosis, which causes considerable scarring, blocked fallopian tubes, and damaged ovaries, experience the most difficulty becoming pregnant and often require advanced fertility treatment.”
On the treatment, she said: “Endometriosis needs the female hormone estrogen to develop and grow. Birth control pills and other drugs that lower or block estrogen can be effective in improving pain symptoms. For patients who wish to become pregnant, medical therapy may be considered prior to attempts at conception, but this treatment usually does not improve pregnancy rates.
“The combination of surgical and medical therapy may be beneficial in patients attempting to conceive through in vitro fertilisation (IVF). Overall, treatment is highly individualised for each patient.
[ad]
“Surgical excision of endometrotic cysts or tissue is recommended while adhesion may also be surgically removed, in an attempt to clean up the pelvis. All surgeries can be carried out by operative laparoscopy/laparotomy.
“Hormonal treatment is also available to suppress the chronic irritation and cysts caused by endometriosis. Danazol, progesterones, oral pills and GnRH analogues are some useful drugs. In mild endometriosis, ovulation induction and intra-uterine insemination may be considered. Otherwise IVF treatment is usually indicated.”
In his presentation at the maiden endometriosis conference in Lagos tagged ‘Endometriosis 101’, the Acting Head, Department of Obstetrics and Gynaecology, Lagos State University Teaching Hospital/College of Medicine (LASUTH/LASUCOM), Dr. Abidoye Gbadegesin, explained that endometriosis affects girls and women of reproductive age. Gbadegesin was represented at the conference by Dr. Temitope Odetayo, a senior registrar.
The Director of Nursing Services (DNS), Lagos State Ministry of Health, Dr. Dorcas Shonibare, encouraged health practitioners to work with focus groups and organise educational programmes that would not only raise awareness about endometriosis but also equip the people with relevant information they need to deal with the condition.
The health intervention and programmes evaluation expert said “while it is important to seek government’s assistance with such projects, it is a call to duty for everyone to strengthen informal and formal groups that can tackle the issue of endometriosis awareness”, noting that “education, not income is the best predictor of a long life.”
[ad]

