 Follow Us on Google News
Follow Us on Google News Follow Us on Google Discover
Follow Us on Google Discover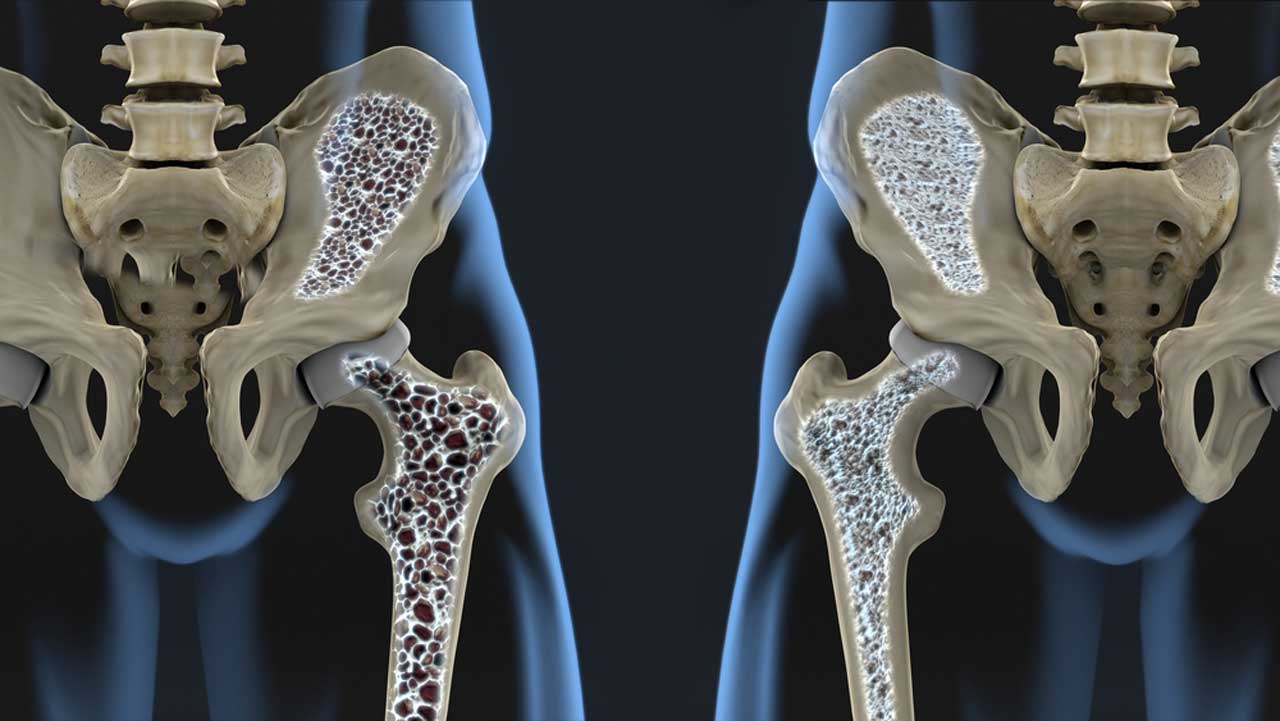
Dr. Akinsulire Adewole is a Consultant orthopaedic and trauma surgeon in the Spine/Oncology unit of the Department of Orthopaedics and Trauma, Lagos University Teaching Hospital. He shed light on bone diseases in women, causes and preventive measures. Geraldine Akutu reports.
What specific bone diseases afflict women?
Most bone diseases affect male and female in equal proportion. A few diseases, however, occur more in either of the sexes. Osteoporosis, which is a metabolic bone disease, tends to occur more often in women than men. Osteoporosis is a bone disease, which occurs when the body loses too much bone mass, leading to weakened bones, which predisposes to fractures. It is defined as a reduction in the bone mineral density of a patient to two standard deviation of the local population. The disease occurs predominantly in women, where about 70-80 per cent of people with osteoporosis are women. Osteoporosis can be postmenopausal or secondary (other conditions which affect bone mass and estrogen levels).
What are the risk factors for osteoporosis?
The risk factors for postmenopausal osteoporosis include a family history of osteoporosis, early onset of menopause, nutritional insufficiency, chronic lack of exercise. Race also has a role to play, as Osteoporosis is less common in blacks compared to Caucasians and Asians. Cigarette smoking and alcohol abuse are also risk factors. Thin women with small frames are more likely to develop osteoporosis.
Why does it affect women?
To understand this, we must know how bone is laid down. The bone is a living tissue that is constantly being built (bone formation) and broken down (bone resorption). The net rate of bone formation to bone resorption determines if the bone mass increases or decreases. At birth, the rate of bone formation is more than that of bone resorption, which leads to a net increase in bone mass. This is markedly increased at puberty to age 30, where there is a net gain of three per cent every year, until the bone reaches a peak bone mass at 30yrs. This peak body mass is common to both sexes.
[ad]
At the age of 30, men have five to 10 per cent more bone mass compared to females. What can affect the rate of bone deposition include diet, exercise, genetics, and hormonal and environmental factors. Hormones, such as estrogen and testosterone are protective and help to maintain the bone mass. However, from the age of 30, there is an increase in the rate of bone resorption compared to bone formation leading to a reduction in bone mass. The rate of bone breakdown is 0.3 per cent per year in males and 0.5 per cent per year in females.
However, at menopause (around 50 years) which corresponds to a period of reduced/absent estrogen level, the protective effect of estrogen is removed and bone loss in women accelerates to three per cent per year, leading to a marked reduction in bone mass. The weak bones make women more likely to sustain fractures secondary to minimal trauma.
It is important to note that while bone loss is a natural part of ageing, not everyone will lose enough bone density to develop osteoporosis. There is a borderline between normal bone and osteoporotic bone, which is called osteopenia. By age 65 to 70, the rate of bone loss slows down, such that by 75 years, it is 0.5 per cent every year. Curiously, a similar thing occurs in males, but the phase of rapid bone loss occurs about 15 to 20 years later than women, which is 65 to 70 years.
What are the signs of bone diseases in women?
Osteoporosis is a silent disease and doesn’t give any symptoms until it leads to a fracture. Many times, the fracture is the pointer to there being osteoporosis. The commonest sites of these fractures are the wrist, the spine and the hip. These fractures may occur with little or no trauma. Common symptoms are a woman in menopause, who develops back pain or a back deformity. There may also be a reduction in the person’s height due to multiple vertebrae fractures. Some women may present with fractures usually of the wrist or the hip following a low energy fall. Unfortunately, women who have a low energy fall have twice the normal risk of developing another.
What age range experiences these diseases?
Post-menopausal osteoporosis generally affects women after 50 years of age. However, secondary osteoporosis can occur at a much earlier age. These are conditions that cause reduction of estrogen production in women, usually before menopause. They may also cause reduction of bone mass independent of estrogen levels. They include women who have undergone oophorectomy, which is removal of their ovaries, prolonged corticosteroid use, inflammatory disorders such as rheumatoid disease. Excessive alcohol, smoking and chronic renal disease are some other conditions that may cause secondary osteoporosis. These conditions can make osteoporosis manifest at an earlier age than post-menopausal osteoporosis.
Genetics play some role in osteoporosis, as some women with osteoporosis might also have a family history of it occurring in their mother or relatives. This exact effect has not been fully determined, but it is thought to be due to a change in the rate of bone breakdown and bone deposition.
Can it be detected?
Features might be seen if a patent does an x-ray for another reason and the bone looks osteopenic. The patient is subsequently further evaluated. Most patients present with the sequela of osteoporosis, which is fracture usually of the wrist, spine and hip. Where osteoporosis is suspected, the confirmatory test is a DEXA (Dual Energy X-ray Absorptiometry) scan, which is used to measure bone mineral density. It compares the bone density of the individual to that of the local population. If an individual falls to two standard deviations below that of the local population, a diagnosis of osteoporosis is confirmed. If an individual has a reduced bone density but not up to two standard deviations of the local population, it is termed osteopenia.
What treatment options are available?
Treatment should be as directed by a qualified medical professional. Treatment options include various medications, such as bisphosphonates, which reduce bone loss and fracture risk and may also help to build bone density. The use of hormone replacement therapy has reduced due to concerns about risk of cancer and blood clots, among others. Dietary supplementation of calcium and Vitamin D also helps to improve bone mineral. Taking a diet with high calcium and Vitamin D, i.e. milk, cheese yoghurt, fish such as salmon and tuna helps bone formation. Once fractures have occurred, they should be treated by qualified specialist, and care is usually individualised based on the patient’s conditions.
What measures can be taken to prevent osteoporosis?
With the knowledge of how bone is lost or gained, if one can achieve peak bone mass before bone resorption, one will reduce the risk of osteoporosis. A good diet rich in calcium and vitamin D, regular weight bearing exercise i.e. walking, jogging, running and nutritional supplements are important. Similarly, reducing or stopping smoking, excessive alcohol intake and unnecessary steroid use can also help reduce the risk of osteoporosis.
[ad unit=2]

