I have cooperated with other colleagues across the country to write two professional books for the use of our students and professionals in Medicine and other relevant health professions. I have actively pursued standard curriculum development and execution till date. I have had the opportunity to lecture at various times as Associate Lecturer, full-time Lecturer and/or Adjuncts Lecturer/Professor in many Universities in Nigeria including University of Ilorin, Benue State University, University of Calabar, Ekiti State University, Bingham University, Afe Babalola University and University of Medical Sciences.
I have also lectured Postgraduate Doctors during revision courses organized by the National Postgraduate Medical College of Nigeria. The response from my students has always been that of enthusiasm and appreciations. (Odimayo et al 2010;Odimayo and Nwokedi (Eds)2014; Odimayo (Ed) 2016).
Respected Ladies and gentlemen, we just have to keep the pace of studies. Because if we don’t do it, some other persons may also fail to do it and that means suffering for our people. So we study common microbial agents responsible for many diseases and their antibiotic sensitivity pattern included in the list are: Agents of female genital discharge(Nwadioha et al 2009).Where we found the commonest being Candida species in 42% of cases, next to which was Gardnerella vaginalis.
Trichomonas vaginalis and Neisseria gonorrhoea were rarely isolated. Studies on Bacteria agents of Acute Pneumonia in HIV seropositive patients showed that Streptococcus Pneumoniae was still the commonest followed Pseudomonas aeruginosa (Nwokedi et al2009),Inour comparative study of bacterial isolates from the urine samples of AIDS and non-AIDS patients in Benue, Nigeria, we found no difference in the sensitivity pattern of agents causing Urinary tract infection in HIV and non-HIV patients. However, HIV positive patients had wider spectrum of organisms such as candida species, Pseudomonasaeruginosa,(Okwori et al 2010). In our bacterial isolates in blood cultures of children with suspected septicaemia in a Nigerian Tertiary Hospital(Nwadioha et al 2010),we found Escherichia coli was the commonest Gram negative while Staphylococcus aureus was the commonest Gram positive bacterial agent.
We found a low prevalence of Urinary Tract Infection(UTI) among Children newly diagnosed with Primary Nephrotic Syndrome and Acute Glomerulonephritis (Adedoyin et al 2010).Antibiotic sensitivity testing of clinically significant bacterial isolate in Ilorin(Odimayo et al 2011).Bacterial Isolates in Blood Cultures of children with suspected septicaemia in Ilorin, Staphylococcusaureusw as the most common isolate, followed by Salmonella species (Adedoyin et al2013).In a cross sectional study conducted to determine the epidemiology and antibiotic sensitivity pattern of bacteria isolated from blood cultures of septicemic patients in Ekiti State University Teaching hospital, Ado Ekiti, commonest isolates were Staphylococcus aureus, Klebsiella species and Enterococci (Nwadioha et al 2015).
Other studies conducted to determine agent of infection in various sites and their sensitivity pattern include microbiologic review of seminal fluids; Antibiotic Profile of Urinary Pathogens; antibiotic sensitivity profile of E. coli associated with specific infections. Evaluation of Uropathogens in Bladder Outlet Obstruction Secondary to Benign Prostatic Hyperplasia (Nwadioha et al 2016, Odimayo et al 2016a, Odimayo et al 2016b, Adegun et al 2017).
Our contributions in the identification of agents responsible for specific diseases and their antibiotic pattern is central to early and effective commencement of therapy for patients with infectious diseases in order to save lives. It is also invaluable in the development of antibiotic prescription policies in our hospitals. In general, we found alarming increase in resistance of bacterial agents of infection to common antibiotics from 2006 till present.
Our various studies and that of others have shown 60 to 87% resistance to common antibiotics in our environment. These are caused majorly by misuse of antibiotics, yet 59.9% of drug sellers consistently sell antibiotics to buyers without doctors’ prescription. Currently, out of pocket (OOP) expenses for health care by Nigerians is among the highest in the world (Federal Ministries of Agriculture, Environment and Health 2017; Awosan et al 2018).
Mr Vice Chancellor Sir, Late in 2007, we did a retrospective study to determine the seroprevalence of Hepatitis B viral infection among patients attending Aminu Kano Teaching Hospital in Kano metropolis using hepatitis B surface antigen (HBsAg) as a marker. Over the 3 years period, a total of 6,395 patients comprising of 4,040 males and 2,355 females including adults and children tested for HBsAg from January 2004 to December 2006 were analysed. Among these patients, 703(11.4%) comprising of 240 (10.2%) females and 490 (12.1%) males were positive for HBsAg. The highest prevalence was seen at the extremes of life in which 19.4% and 16.9% were seen among patients below 10years and above 50 years respectively.
The yearly trend of HBV surface antigenemia was 220 (14.6%) in 2004, 235 (10.1%) in 2005 and 275 (10.7%) in 2006. We concluded that the prevalence of HBsAg among patients attending Aminu Kano Teaching Hospital, Kano was high and highest prevalence was seen at the extremes of life. The presence of hepatitis B surface antigen (HBsAg) in the serum of an individual indicates carrier state or active acute or chronic infection with hepatitis B virus. The presence of hepatitis B surface antibody (HBsAb) usually indicates resolved infection or following effective hepatitis B vaccination. We went further to assess the HBV situation in Makurdi. Our target was on the community. This we did through multiple Hepatitis B Virus health education and screening activities in Makurdi.
This stem from an initial pilot study which showed a high prevalence of HBV in Makurdi, Nigeria. The series of community screening were conducted between April 2008 and June 2009. We reviewed a total of 676 individuals consisting of 430 males and 246 females screened for hepatitis B virus using HBsAg as marker and a community prevalence of 12.7% with a male to female ratio of 2.3: 1 was discovered.
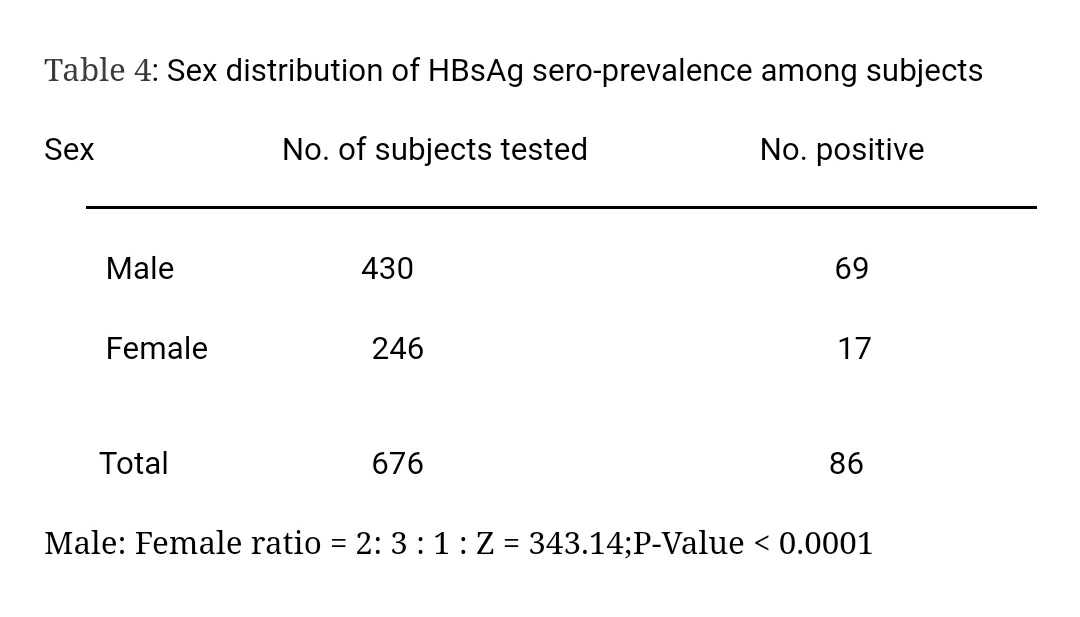
Highest rate of 21.2% rate was found among the 30-34 years age group. That was a very high prevalence and showed that the infection was more common among young adults and middle aged individuals with significant male preponderance. We therefore recommended mass screening among the populace, appropriate treatment for infected individuals and immunization of Hepatitis B virus negative individuals irrespective of age and occupation. We successfully screened and vaccinated thousands of people in Benue state. Many infected individuals were further evaluated and treated as appropriate. We continue to pursue the mission of control of hepatitis B virus through health education, vaccination and treatment till date.
In the course of practice as a Consultant Microbial Pathologist, a few cases of liver cancers were seen among middle aged individuals. All of those seen were positive for hepatitis B virus for variable duration of time. Such patients are normally referred to relevant Consultants. However, knowing the fate of such patients in term of short life expectancy, we were moved to further pursue the control of HBV in our society.
Therefore from determining the prevalence of hepatitis B viruses, we went further to see the prevalence of those individuals whose infection is aggressive enough to possibly result in cancers or result in increased HBV transmissibility. Hepatitis B e antigen is a marker of aggressive HBV infection. We had to settle for that because of the cost of HBV viral load which was prohibitive and difficult to come by in our environment.
We determined the prevalence of Hepatitis B ‘e’ Antigen (HBeAg) among hepatitis B surface antigen positive patients in Makurdi, Nigeria. We found that among 467 patients screened for HBsAg, aged 0-65 years from July 2009 to February 2012 in Delight Specialist Clinic and Maternity, Makurdi. A total of 96 was HBsAg sero positive. Among the HBsAg sero positive patients, only 3(3.1%) was HBeAg positive. All(100%) Hepatitis B “e‟ Antigen sero-positive patients were under age of 22 years.
The study showed a low seroprevalence of HBeAg in a high hepatitis B sero-positive endemic population with adolescent age posing a higher risk for HBeAg.HBeAg is a marker of aggressive hepatitis B viral disease and possibly of liver cancer development. The next question was, why was ‘e’ antigen so low in our environment with high HBsAg seroprevalence and endemic liver pathologies? Other plausible explanation had been given by You et al (2004)that HBV mutations may result in ‘e’ antigen gene deletion and yet be aggressive with risk of hepatocellular carcinoma. Since hepatitis B viral load was difficult to achieve, we decided to focus on other HBVserologic markers (Odimayo MS et al 2010, Nwokedi et al 2011, Odimayo 2013)
After many years of active HBV campaign. We needed to know if our campaign was making impact. This was done through a cross sectional survey conducted on HBV awareness among members of Benue State University community in Makurdi, Benue state, Nigeria. A total of 728 individuals were recruited into this study consisting of 308 (42.31%) females and 420 (57.69%) males. Our subjects came from different parts of Benue state and beyond. Majority (63%) were between 21 and 30 years of age. Over 90% of the study group attained up to tertiary level of education; about 30% were married.
We found that there was a significant awareness of hepatitis B virus infection among the study population as 81.1% had heard of HBV. However, some misconceptions which can result in stigmatization of HBV infected individuals existed. We recommend the strengthening of ongoing Health Education programs on HBV in our environment (Odimayo et al2015)
Since Hepatitis B Viral DNA load determination was difficult to achieve on routine basis for general diagnostic and treatment purposes. We thought of ways round it. How can we diagnose HBV and determine need for treatment or otherwise without viral loads for all patients. Fortunately, more serologic tools as diagnostic markers were becoming more available but the interpretations were complex. We moved ahead to determine the pattern of HBV serologic markers in HBV surface antigen (HBsAg) seropositive patients. HBsAg seropositive patients were screened for other HBV serologic markers namely, antibody to HBsAg (HBaAb), HBV e antigen (HBeAg), antibody to HBeAg (HBeAb) and antibody to HBV core antigen (HBcAb). Liver enzymes (AST and ALT), age, sex and complaints of subjects were also documented.
Sixty three HBsAg seropositive patients consisting of 65.1% males and 34.9% females with age ranging from 15 to 80 years were enrolled. Majority (70%) was between 20 and 40 years. We found that all patients with HbsAg seropositivity were sero-negative for HBsAb. Among the 5 patients (8%) which were seropositive for HBeAb, 2 of them were also HBeAg seropositive. HBcAb seropositivity was 95.2% (n=60/63). Serum transaminase enzymes level was normal in 80% of patients. Commonest complaint (over 80%) was upper abdominal pain. We concluded that in absence of Hepatitis B Viral DNA load determination, understanding of serological markers of HBV is important in the management of patients with chronic HBV infections. With appropriate literature reviews, we discovered that most of our HBV seropositive patients actually requires treatment because they were symptomatic and positive for core IgM immunoglobulin (HBcAb)(Odimayo et al, 2016). Further study in this direction among blood donors confirmed that HBcAb was the only marker that correlated with detectable viral loads in occult HBV infections (Nwadioha et al 2018).
We are currently working on comparing the serologic pattern with viral load. This is very important to allow us to correlate viral load with HBV profile with a high degree of certainty in order to help our patients who may not be able to afford viral load determination. This is of serious concern. The second most important point of study is the determination of HBV genotypes circulating in our environment as this is important to determine response to therapy and prediction of complications. We are doing a lot of underground work to achieve this. We look forward to opportunity and support to commence studies in this direction.
Other research efforts at HBV showed that our Health care workers (HCWs) are still particularly at risk of hepatitis B virus (HBV) infection due to contact with infectious material like contaminated blood and body fluids or contact with HBV contaminated fomites. And that routine vaccination of HCWs is often not implemented due to cost in our setting. A cross-sectional study conducted among Staff from various cadres in EKSUTH, Ado Ekiti showed that among a total of 965 participants, 43(4.5%) were HBsAg positive out of which 40 (93%) had HBV infection as predicted by HBcAb seropositivty. Prevalence of HBV infection was significantly higher among males than females. Majority (60.5%) of infected individuals were 30 to 49years of age.
None could afford viral load testing. All infected participants had no previous vaccination. We concluded that Hepatitis B virus infection is still high among HCWs and significantly higher among males than females. Vaccinated individuals were found to be HBsAg negative but had no detectable protective immunoglobulin against HBV. We recommended pre-employment screening and continuation of free vaccination for all staff in our health institutions. In addition, post vaccination immunization status should be determined. There should be provision of standard and affordable treatment for infected individuals (Odimayo et al 2018). Currently, quantification (not just detection) of HBsAg has been found valuable in the assessment of treatment needs of patients. This should be available in the next few weeks within the Microbial Pathology Laboratory of UNIMED for the benefits of our people.
Our next target is affordable solutions to HBV in our environment. We have created awareness to thousands of individuals, vaccinated thousands and commenced treatment for many of our people. We just must keep up efforts at reducing the prevalence of the disease as the global community is working at elimination of viral hepatitis by 2030. Currently the effort at this major milestone is on as the University of Medical Sciences is about to install our hepatitis B viral load quantification equipment to enhance HBV molecular diagnosis. The work is in progress.
As the world is making efforts at identifying advanced methods of diagnosis which are often cost prohibitive to our people, we strongly feel that if we can establish affordable means of effective diagnosis and management of our patients, we would have met the need of our teeming populace. This we believe should be the focus without losing track of advanced technologies at the research levels. Global efforts at the control of infectious diseases is amazing.
In the last International Viral Hepatitis Elimination Meeting (IVHEM) held in Amsterdam, the Nether lands in December, 2019; We observed that most nations of the world are approaching elimination faster than you can imagine. For example, Hepatitis C virus is now fully curable while effective treatment protocols for Hepatitis B virus have been developed. It is vital to follow global plan as we develop more cost effective techniques.
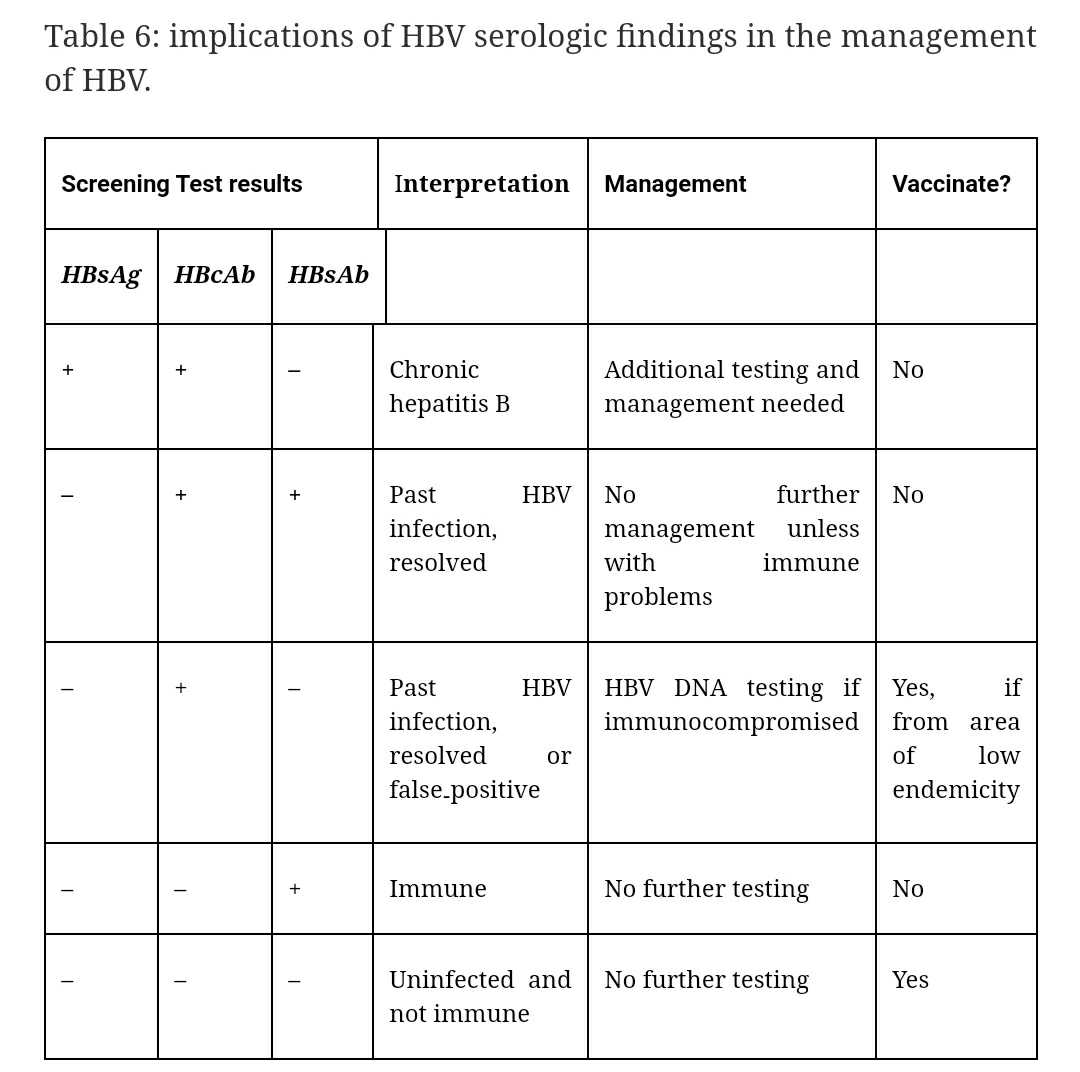
Several steps are essential to guide initiation of HBV treatment and to evaluate patient response during antiviral therapy in patients. Please observe that in the diagnosis of chronic hepatitis B viral infection, serologic testing is substantially useful as presence of HBcAb and absence HBsAb in HBsAg seropositive individual shows chronic infection (Table 6).
The decision to treat versus monitor Chronic hepatitis B Virus patients should be based on clinical features, serumALT level, HBV viral DNA load, determination of liver architecture by liver biopsy or Ultrasound. The above indicators give information on viral replication and extent of liver damage. Extent of viral replication is measurable by viral load while extent of liver damage is determined by using ALT levels, or structural damage of the liver as shown either through invasive tests like liver biopsy or non-invasive procedure such as transientelastography(Yang et al 2014; Terrault et al 2018). HBV DNA is typically measured quantitatively via real-time polymerase chain reaction methodology. The presence of cirrhosis is an indication for treatment. Non-invasive evaluation of the liver can also include risk calculators based on serum markers (Yang et al 2014; Terrault et al 2018). The upper limits of normal for ALT defined in four international guidelines are as shown in table 7.
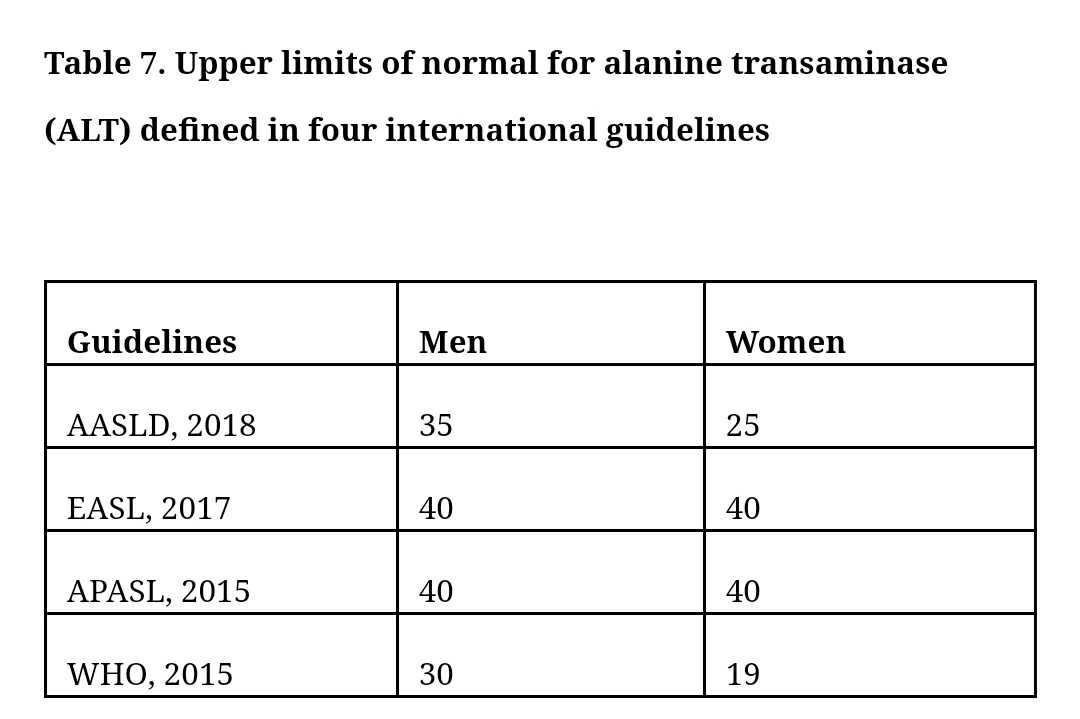
The American Association for the study of Liver Disease (AASLD), recommended that the upper limit of normal (ULN) for ALT in healthy adults is 29-33 U/L for men and 19-25 U/L for women. In Nigeria, upper level of normal for ALT to 6.42-14.06(Christiana et al 2015).To guide treatment, the AASLD uses an ULN of 35 U/L for men and 25 U/L for women. Correlation of HBV serologic profiles with the state of the liver and aggressiveness of the disease is our current research focus. This we believe if achieved, will significantly reduce the cost of management of the disease among our people. In addition, the accuracy of Transient Elastography (TE) in the diagnosis of cirrhosis in patients having chronic hepatitis B and C is very high and the procedure is perfectly safe (Jing-Houng Wang 2019). In summary, diagnosis of viral hepatitis for treatment is complex in the phase of different types of chronicity like obvious infection (overt) or masked infection (occult) and carrier states (Alavian & Miri 2011; Alavian2012; Pourkarim et al 2014).
PCR for viral load determination and ELISA for surface antigen quantification is almost ready in Microbial Pathology of UNIMED/UNIMEDTH for effective diagnosis and treatment. We are currently working with our international friends for the incorporation of Transient Elastography (TE) to further enhance the effectiveness of the team. About a year ago, a high powered team of researchers with varying backgrounds formed a cancer research team. We have developed proposal that will allow us to effectively investigate many of our local capabilities for the treatment of cancers. We hope to make a lot more progress this year as we call on well-meaning institutions, organizations and individuals to support this great initiative that has the capability of turning our nation to a net exporter of anti-cancer remedies.
Efforts at excellence is usually embellished by knowledge. In the last one year, I commenced a postgraduate diploma program in Administration. It is a good opportunity to learn the management of resources and people. I have already completed the course work with multiple distinction grades. I appreciate the Vice Chancellor for the encouragement I got from him. He is a darling indeed. As we move towards conclusion of this lecture, I wish to appreciate the Federal Government of Nigeria for the inclusion of hepatitis B vaccine in the National Program on Immunization (NPI). Hepatitis B vaccine has been introduced into NPI since 2004.
Our recent study on the prevalence of HBV infection and sero-conversion status among immunized cohort of children was conducted in Ekiti state, Nigeria. Among a total of 441 children who had been vaccinated before the age of 1 year, all (100%) were negative for HBV infection. This is a cheering discovery. However, we found that only 10.7% of the subjects had detectable HBsAb after 5-10years following initial vaccination. This shows that majority of these children may be at risk of HBV at a later age and we recommended a booster dose of hepatitis B vaccine at the school age of 6years to all children. We are about to commence a quantitative measurement of the protection to further substantiate our initial findings. Further findings on continued work on this will be reported soon (Odimayo et al 2019).
CONCLUSION
Above is a tip of the iceberg on what a Microbial Pathologist can do in turning the tides against infectious diseases. The relationship between humans and microorganisms has been that of the good, the bad and the ugly. As written in the bible in Genesis 1: 28,
‘’And God blessed them, and God said ……….replenish the earth, and subdue it………….’’ KJV
Our ability to subdue microorganisms as a component part of the earth means we should know and understand microorganisms so well as to be able to adapt them for guaranteed safety of lives and utilise them for human good.
This is not yet the case as we currently have an alarming resistance of bacteria to available antimicrobial agents. There are multiple resistance bacterial such as: Extended Spectrum Beta Lactamase (ESBL) -producing Enterobacter spp, Methicillin-resistant Staphylococcus aureus (MRSA) and carbapenem-resistant Acinetobacter spp now commonly isolated. This is because of inappropriate use of antibiotics. Yet the practice of antibiotic usage without medical prescription is still heavily prevalent in our environment. What are we doing to ourselves?
The cost we thought of saving by liberalizing drug usage is being eroded by loss of precious lives and heavier cost of healthcare delivery. We all have to pay more by having to buy very expensive antimicrobial drugs as it is today. We must act fast and urgently too. Hospital Acquired Infections is still in our hospitals, the rules have not changed? With appropriate committees and supports, we can life a lot better for our patients.
The problems of malaria in terms of diagnosis, treatment and prevention is still a big issue. However, the solution, as My Vice Chancellor, Professor F. E. Okonofua often says, ‘is a low hanging fruit.’ This is because the gold standard for malaria diagnosis using microscopic examination of stained thick and thin blood film as stipulated by WHO has not changed. And the use of insecticide treated nets in prevention of malaria is still quite effective.
The impact of the health sector on the health and wealth of Nigerians is unquantifiable. However, the leadership struggle and animosity within the health sector is giving way to anarchy, mutual suspicion, laxity and loss of lives of our precious people (patients).This is speedily destroying the health sector. Healthcare delivery is being destroyed! This is a wakeup call. All hands must be on deck. The efforts of our government at supporting the health of the people including vaccination of all children against hepatitis B virus is commendable. However, we must be conscious of the heavy presence of viral hepatitis in our nation. And also realise the complexity of diagnostic algorithms for management of cases. With a population of about 200million people, the current prevalence of 12. 4% means over 20 million people are infected. Yet, only a handful of infected individuals are accessing standard treatment.
Although the eradication of hepatitis B by means of universal vaccination seems technically achievable, this task is made difficult by the hundreds of millions of individuals who are already chronically infected with HBV globally. The elimination of hepatitis B will only be successful when this group of chronically infected patients are cured. This we are seriously working on in UNIMED/UNIMEDTH as our Viral diagnostic system is about to be fully installed.
Rotavirus is still a major killer of our children. The federal Government of Nigeria has promised to incorporate vaccination against rotavirus into our National Program on Immunization.
RECOMMENDATIONS
A lot needs to be done to support Pathologists in the health sector. In fact, all departments in Pathology (Laboratory Medicine) is endangered with serious negative implications on the advancement of medical practice in Nigeria. There are various encroachments, legislations and negative manipulations against Pathologists. This is worse in Microbial Pathology discipline. And our nation is paying dearly for these with inefficient diagnosis of diseases and loss of human and material resources. Worse still, the effects of such is a reduction of interest of younger colleagues in Pathology specialties thereby limiting the contribution of our nation to advances in global field of Medicine. I call on our National assembly to seriously look into the practice of Laboratory Medicine in Nigeria. The nation is sitting on a keg of gun powder and something serious must be done to restore peace in the practice of Laboratory Medicine in Nigeria!
Today, multiple agitations, inter and intra professional rivalries and disruption of rules and order in the health sector and especially in departments located within Laboratory Medicine has almost grounded the health sector. We can do much better. I appreciate God for our Vice Chancellor, Professor F. E Okonofua for his wisdom in handling this in UNIMED. I have closely studied him and learned so much from him after working with him for this long. Today, such wrangling does not exist in UNIMED. This has made us to work together for a greater UNIMED. My friend, Dr Abubakar Abdulazeez of Medical Laboratory Science department can attest to this. In addition, our friends in Nursing, Physiotherapy and other departments can also testify to his unifying capability worthy of full acceptance and emulation. It is clear that a Medical Doctor is the leader in any Medical Practice.
That notwithstanding, the importance of every participant cannot be underestimated and the value of mutual respect and understanding at all times cannot be overemphasise. Therefore, nobody should be taken for granted. It is also very important to note that good leadership and respect for constituted authority coupled with appropriate job description and adherence to job specification is very vital for effective healthcare delivery. Above all, friendship should be cultivated across board because mutual relationship benefits all. If harmony is achieved in the health sector, then the fabrics of Laboratory Medicine practice which is premised on correct diagnosis and excellent turn-around time can be achievable for the good of our people.
The practice of medicine requires careful use of available medications. This is especially important in infectious diseases in order to slow down resistance. Practice must follow the standard as laid down to avoid undermining available medications. Under dosage or treatment for inadequate duration results in a monster called resistance. In the face of resistance, cheaper drugs that have been abused becomes ineffective and as such the society pays mare in the purchase of more expensive drugs. This is even worse when the society encourages self-medication and quackery as the society ends up paying exorbitant price for other drugs which are often very expensive and associated with more side effects. As long as Medical practice is undermined by free and open market of antimicrobial drugs in this country, resistance will continue to rise with increasing cost of healthcare at individual and national levels. We therefore need to step up regulations to stem the negative effects of quackery in our community,
Insecticide treated nets (ITNs) is highly advantageous in the prevention of malaria, I encourage everybody in this hall to get for every member of his/her family. Make it part of your room beautification agenda. There is also need for aggressive promotion of the use of ITNs through marketing and health education. Tuberculosis of the uterus is rare but occurs. With the current availability of assisted fertility in our environment, a lot of families have been saved from the bitterness of divorce resulting from childlessness. Even at this, we should look out for TB of the uterine tubes as failure to identify this in an individual with such condition is intimately linked with sterility. There are available screening tests for early diagnosis and this should be included in the battery of investigations in infertility cases.
The problem of hospital acquired infection should be of concern to all stakeholders in the health sector. The Microbial Pathologist is central from the pathogenesis, to the wards and into the laboratory. I hereby encourage our hospital management to make it a matter of concern. There should be establishment and supports for Infection Control Team (ICT). ICT is usually headed by a Microbial Pathologist with the incorporation of nurses and medical laboratory scientists in effective prevention of HAI. In addition, Infection Control Committee usually headed by the Chief Medical Director (CMD) should be on ground to support the ICT. The impact of rotavirus vaccination to children especially in the first year of life cannot be overemphasised. With the introduction of the vaccine alone, about 160,000 childhood deaths could be averted annually. The Federal Government of Nigeria should endeavour to make do their promise by incorporating rotavirus vaccination into the National Program on Immunization unfailingly in this year 2020.
A recent average national prevalence of HBV was found to be 12.7%. Considering a population of about 200 million people, this implies over 25 million Nigerians have hepatitis. Yet, the health seeking attitude of infected individuals is very poor. In our most recent studies (unpublished) in Ondo state, less that 10% of patient diagnosed positive for hepatitis present for follow up and treatment. Among those who came for follow up, less than 25% showed enough commitment as to do viral load and other tests to qualify for commencement of treatment. Yet the global target for viral hepatitis elimination is 2030. This shows the need for more of governmental, NGOs, community and individual commitment to viral hepatitis elimination. Individual screening, vaccination and treatment should be encouraged to reduce the premature deaths associated with the disease. Efforts should continue to be made in correlating viral loads and other clinical parameters with HBV serologic profiles in order to reduce the cost of patients’ management of HBV.
Vaccination of HBV seronegative individuals in our environment will decrease transmission to health personnel and our people in our communities. Installation of various equipment for viral loads, HBsAg quantification, and liver biopsy is almost ready and more effective and accessible management of viral hepatitis will soon be made available in UNIMED in conjunction with out Teaching Hospital. I recommend that individuals with the diseases should make themselves available in order to save their lives and those of other members of our society. More encouragement is still needed by our various chief executives, our government and other stakeholders to support global viral hepatitis elimination. Please be reminded that hepatitis C virus is curable. Let the good news spread.
AKNOWLEDGEMENT
I will sing unto the LORD, for He has triumphed gloriously: the horse and his rider hath he thrown into the sea Exodus 15:1. May God’s great name be praised for ever amen?
To my Spiritual fathers, Pastors E.A Adeboye, Bishop Oyedepo, W. F Kumuyi and all the men of the great God who have lived the lives of discipline, sacrifice and dedication to God thereby illuminating the nation. You refused to give room to the devil, thereby making yourselves examples of good work. Thank you Daddies. You taught the youth under your leadership to understand the values of national peace and prosperity in the fear of God. You are great indeed. How I wish all leaders will be like you and great will be the peace and prosperity of our land! To my Regional Daddy, Pastor Idris UmarEnoch, thank you for your excellent leadership and love. To My Provincial pastors, Pastor A. A. Bello, Pastor Ayanbode, Pastor Oyesola. Thank you for your love and prayers. To my Zonal pastors, Pastor Adebayo, Pastor Olumide Fakua and other men of God, Thank you all.
To my Daddy, Chief Andrew Akinyele Odimayo, and my Mommy, Mrs C. K. Odimayo; I bless God for your life, your patience, prayer, discipline and love made me great. I can never thank you enough.
To my Mentor, Friend and Teacher, Late Professor Matthew Akinyemi Araoye, thank you for the trust and confidence you freely gave me. I thank God I never disappoint you. Professor Boaz Adegboro, Professor Anjorin A. S, Professor Charles Nwabuisi, I thank you so much for your selfless dedication to service. Your diligence is major in who I am today. To Professor (Pastor) Adedoyin Olanrewaju, thank you for your trust, Mentioship and spiritual leadership. Your decision to hand over some vital responsibilities to me in trust helped me to live up to and even surpass expectation and changed my view and disposition to God and human service. Thank you Sir. To Professor Taiwo S. S, who positioned himself to challenge me for excellent service in the earliest part of my training as Resident Doctor, I thank you. ProfessorS. S Taiwo was my Chief Resident Doctor and he painstakingly planned and ensure standard training is accomplished earlier in my postgraduate training. I am grateful for your dedication to service. Those days of professional discipline and diligence you, Prof. Buhari M. O and Prof. Oghagbon made me pass through when you were Chief Residents are cherished for life. To my dear and friendly senior colleague, Professor Akanbi II A. A, Professor Olowo Samuel, Professor Babatunde A. S. I thank you all.
My special gratitude goes to Dr Olanrewaju I. Wahab, The Medical Director, Olanrewaju Hospital and Project Director, Malaria Resource Centre, Ilorin for being a wonderful friend, with so much age difference, yet, we interact like childhood friends. He will painstakingly guide and support me, tell me the truth sternly when I made mistakes and support me when need be. We did my first series of work and publications together. He actually introduced me into the world of research early in my career. Thank you so much Sir.
To my friendly colleaques, Dr Fadeyi Abayomi, Dr Jimoh A. K, Dr Ibrahim O.O.K., Dr Shittu, Dr Omotayo, Olaosebikan F. F., among others, I say thank you. Just like yesterday, It was twenty years ago that we started postgraduate Medicine (Residency) at about the same time. We were really together then. Can’t you see the confirmation of the words of our elders, which says ‘twenty children cannot play together for twenty years?’ So are we not able to work together in the same place continuously for twenty years.
To my Dear Friend, colleague and prayer partner, Dr Olanrewaju Olusegun Timothy and your entire family, I am grateful to you for being there all along all these years. God has used you in many instances for me. Many thanks to you. To my dear friends and colleagues, Dr Busari, Dr Mutiu, Prof. Nwokedi EOP., Prof. GTA Jombo, Prof. Nwadioha SI, Dr Duduyemi Babatunde, Dr Akinde, Prof. Ukah CO, Dr Osho PO, Dr Alabi and many others too numerous to be mentioned. Thank you all. To all my international friends including Prof. Jordan Feld, Prof. Charles Boucher, Prof. John Ward, Prof. Funmilayo Lesi, Michael Ninburg, Wang Su, Jean Damascene Makura, David Smookler and a host of others. Thank you all.
On behalf of UNIMED staff and students and all Pathologists in Ondo state, I sincerely appreciate our Governor who have been so supportive to UNIMED by trying his best even amidst very scarce resources. Big thank you to our Arakunrin. You are a performer! Big thank you to my Vice Chancellor, Professor F. E. Okonofua and your entire family, I am grateful for your support and encouragement in the course of my service as Dean, Faculty of Basic Clinical Sciences and as the Chairman of Deans and Directors, UNIMED, Ondo City you are always supportive. You are a great leader with focus, integrity, dedication to service and great strength and fortitude. You are a mentor, a darling and a lifetime friend. I thank you Sir.
We Thank God for our Vice Chancellor, Prof. F. E Okonofua for being proactive and his mastery of the act of judicious use of funds. As it is today, the good people of Ondo state are just about to benefit more from the services of Microbial Pathologists as our Microbial Pathology laboratory for molecular diagnosis in infectious diseases using Polymerase Chain Reaction (PCR) and ELISA are approaching final installations. I give big kudos to our Vice chancellor and our Learned Governor for these feats.
I want to specially thank my very Dear Brother, Egbon and Friend, Professor Arogunjo A.S, The Deputy Vice Chancellor- Academics, UNIMED. Thank you Sir. I will never forget your support and encouragement always. I appreciate you Sir. I treasure your kindness and love. My special gratitude to the entire UNIMED Top Management for the opportunity given me to present the first inaugural lecture of this great university.
To my Dear friends, ‘Egbons’ and associates: Engineer Ade Adetimehin, Honourable Femi Agagu, Hon. Emmanuel Igbasan, Hon Saka Yusuf, Honorable Dr Wahab Adegbenro, Dr Wunmi Ilawole their families and many others too numerous to be mentioned. Thank you for your kindness and love.
To the entire UNIMED staff and students, I love you all. Thank you for your support always. We have a common destiny in UNIMED. As we thank God for the excellent leadership efforts of Professor. F. E. Okonofua, our Government and the entire UNIMED governing Council so far. Our sacrifices and dedication to service has also helped in taking UNIMED this far. This great institution with excellent start shall continue to wax stronger and go greater. In Jesus name.
Big thank you to the Chairman of UNIMED Governing Council, Dr Temitayo Fawehinmi and to all men and women of character and honour in the council. We know your worth. Thank you so much for the work.
To my wife, Mrs Temitayo Janet Odimayo, you are wonderful! I thank God for His favour upon my life to have made you my wife. You are the only one. I cannot trade you for silver, pleasure, honour and gold put together. Because your worth is more than all of them put together and multiplied by a million. You are loving and caring, you are kind and beautiful; you are strong, thoughtful and intelligent. Above all you are honest and true. Thank you! Thank you!! Thank you!!!
To Professor Olu-Aderoumu WO, who took his time to painstakingly edit this manuscript, Thank you so much sir. To my dear Sister and Friend, Professor Roseangela I. Nwumba thank you for your friendly disposition and kind words always. Dr Adaja TM, our able Sub-Dean, thank you for your good advice and readiness to serve at all times. The support of the Faculty Officer, Mrs Awopeju is great, thank you my sister. I cannot forget your diligence and dedication to duty. Thank you for doing your job well at all times. To Catherine, Bukola, Samuel Oguntuase, Ola and many others too numerous to mention, thank you for your supports. You are always available to give your selfless services. I appreciate you. You guys are good!
To all Deans and Directors in UNIMED under the umbrella of Committee of Deans and Directors, thank you for your support always. To all HODs and Professors in the Faculty of Basic Clinical Sciences, I owe you so much for your dedication to service and dispassionate contribution to the growth of our faculty and the entire university. To my HOD, Dr Joseph Adejoke Adijat, our departmental secretary, Mr Ojo and all our dear Technical staff, your contributions are considered precious. To the Resident Doctors in Microbial Pathology department namely: Drs Onogate, Olatunji and Ogedengbe I say big thank you for being part of this family.
To all my Daddies and Mommies present here. See what God has achieved through you! I am here today because of what you did in the past and your commitment to always support. Thank you for being there that time and now. To my Siblings, Brothers and Sisters, CSP Adeknle Emmanuel Odimayo, Fayokemi Odimayo, Ayomibo Odimayo, Oluwakemi Odimayo, Grace Odimayo, Babafemi Odimayo, (including their spouses and children), Peter Odimayo, Teju Odimayo, Modeayo Odimayo, Matthew Odimayo this is your day!
Ladies and gentlemen, thank you all.
Odimayo is Professor of Microbial Pathology/Infectious Diseases delivered this inaugural lecture series 1 in Ondo, recently.